- There are a LOT of sufferers.
- Allergy season is LONG.
- Ocular itch is VERY bothersome.
- Patients are NOT satisfied with solutions.
The size of the prize
It is highly probable that between one-third and one-half of the patients you see in your practice suffer from allergic rhinitis or hay fever.1 In Canada, a survey of 3671 respondents to a phone survey of over 30,000 Canadians indicated that 44% had nasal symptoms unrelated to a cold, 20% had a physician diagnosis of allergic rhinitis, and 27% had used and Rx or OTC drugs to treat symptoms or had a diagnosis of allergic rhinitis and completed the survey questionnaire.2
And more importantly to eye care professionals, from around 50% to over 90% may also experience symptoms of allergic conjunctivitis.3–5 The prevalence of allergies has been increasing during the past several decades. Data from a very large ongoing US study called NHANES (National Health and Nutrition Examination Survey) of people aged 2 months to 90 years found the prevalence for 6 allergens tested by skin prick 2.5 to 5.5 times higher in NHANES III (1988-1994) compared to NHANES II (1976-1980).6
The allergy season is long, and causes are varied
We tend to think of allergy as a spring phenomenon, but allergies can flare up almost any time of the year as different allergens crop up with changes in temperature and wind patterns throughout the year (Figure 1).7
Figure 1: Seasonality of peak pollen production for trees, grass and weeds by province across Canada.
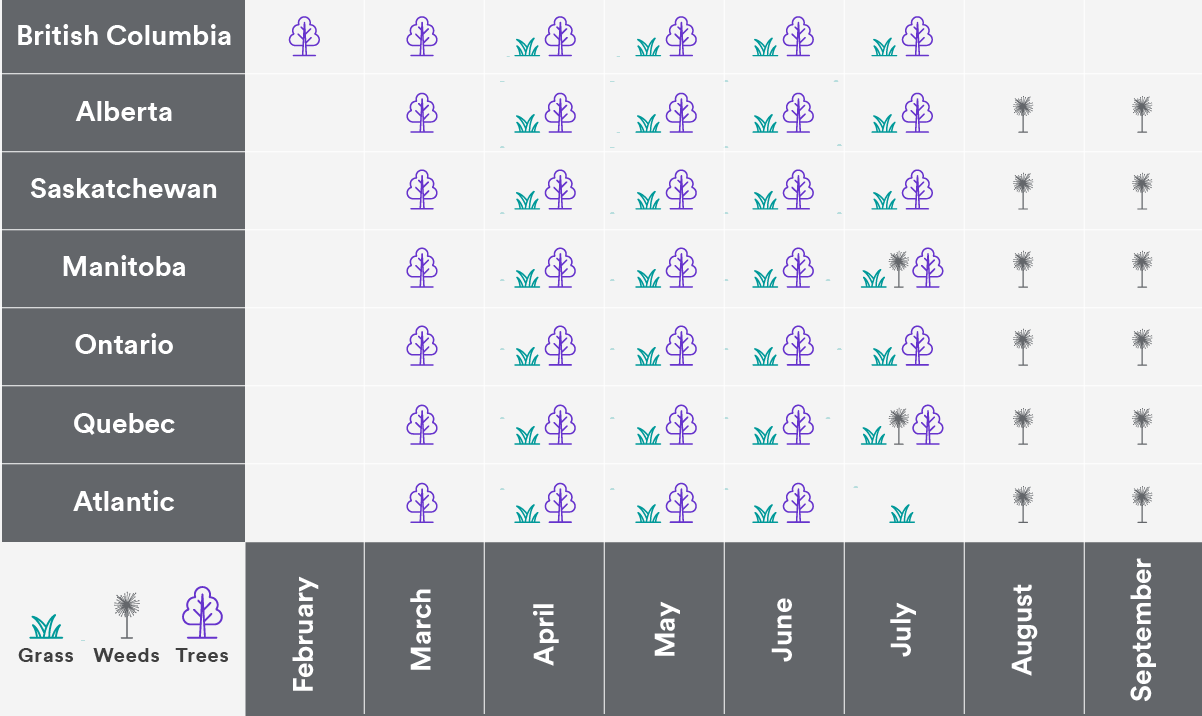
(Source: Quantum Allergy Canada).
In spring, tree pollen predominates. Tree pollen is small, light and abundant and can spread over large distances with the spring winds, which may account for the high rate of allergy suffering in springtime (Figure 2).8,9 It starts early in BC but really picks up from mid-March to mid-June.10,11 The hot dry days of summer see grass pollens peaking, and fall brings weed pollens, with ragweed season stretching from mid-August to the first frost.10,11 And in winter, airborne mold spores can continue to trigger allergies.10,11 In addition, some allergies are more perennial, often driven by indoor allergens such as pets, dust mites, cockroaches and mold.10,11
Figure 2: Seasonality of peak allergy suffering by severity of percent of people suffering. The large peak in spring and minor peak in fall are driven largely by increases in rate of severe suffering.
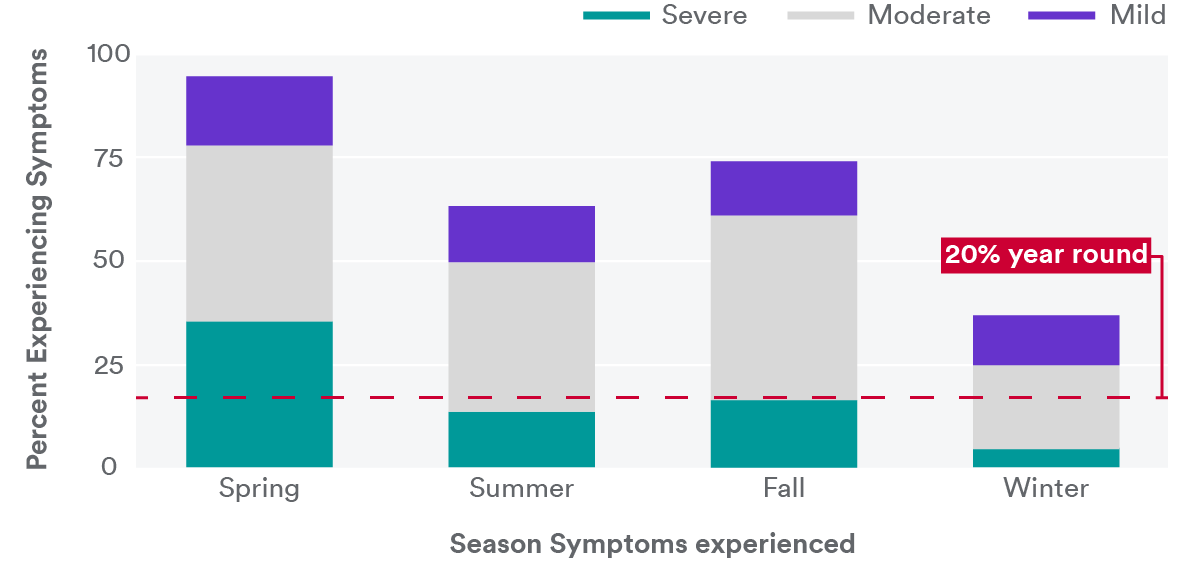
(Source: Meltzer et al, 2017).
Ocular itch is a significant issue!
Ocular itch is not the most frequent symptom of hay fever sufferers but is one of the most bothersome. In a study specifically looking at ocular itch, Stull found that chronic ocular itch was a common symptom affecting 29.5% of patients in the study.12 In another study of over 2700 people in the US, while nasal symptoms were the most common, itchy eyes were #2 in the list of most bothersome symptoms –reported as bothersome or extremely bothersome by nearly 7 in 10 subjects (68%).13 In the Canadian survey by Keith, itchy and watery eyes were in the top 5 of symptoms deemed most bothersome to patients.2 Blaiss and colleagues did a review of the literature in the area of the burden of nasal and ocular allergies found that moderate to severe symptoms was associated with higher odds of having a negative quality of life score (Figure 3). Ocular symptoms in particular were associated with more difficulties, and ocular itch was associated with a large increase in risk of poor outcome for the adolescent group in particular.14
Figure 3: Association between moderate to severe seasonal allergic rhinitis symptoms and poor Rhinoconjunctivitis Quality of Life Questionnaire score in adolescents and adults. Odds ratios were calculated versus the absence of symptoms or presence of mild symptoms only. Moderate to severe symptoms were defined as a mean individual symptom score of 2 or higher during 3 days; poor QOL was defined as a Rhinoconjunctivitis Quality of Life.
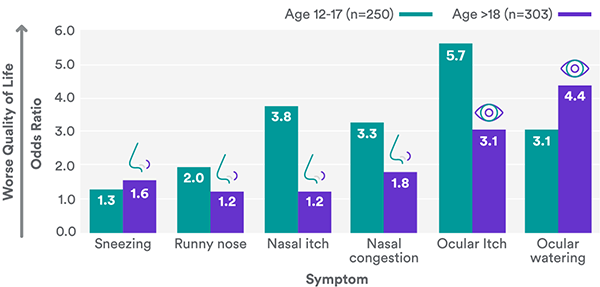
(Source: Blaiss et al., 2018).
Itchy eyes were also the number one symptom reported in driving patients to seek professional medical attention (Figure 4).13 Of note in this study was that not only optometrists and ophthalmologists reported itchy eyes as the primary reason for the visit, but also pediatricians, nurse practitioners and physician assistants. This illuminates an opportunity for eye care professionals to interact with these other health care professionals to ensure they are well informed of the ability of eye care professionals to serve patients in the area of ocular allergies. Bielory, a renowned ocular allergy researcher has stated that the prevalence of ocular allergy clearly is underappreciated and has been under diagnosed and undertreated. He also asserted that the ocular symptoms associated with the most common ocular allergy conditions, such as seasonal and perennial allergic conjunctivitis are TWICE as likely to affect the allergy sufferer rather than nasal symptoms alone.13
Figure 4: Ocular issues reported by 7 different types health care professionals (HCPs) as the primary reason for a medical visit related to allergies.
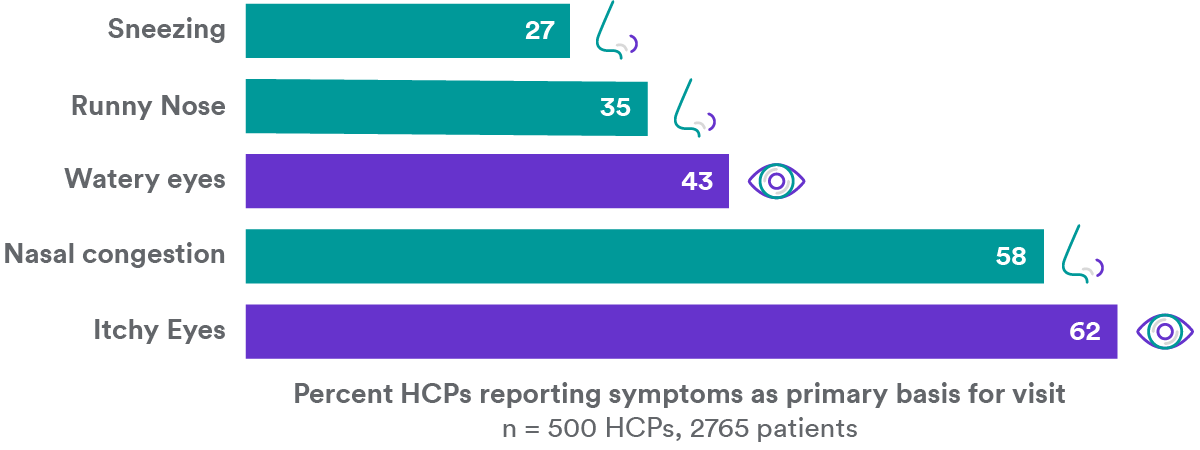
(Source: Bielory et al., 2014).
Allergies make life difficult
The burden of allergies has been studied extensively in several countries. In Canada, 72% of patients indicated that during allergy season their allergy symptoms adversely impacted their daily lives. One quarter to nearly one half of the over 3000 allergy patients surveyed reported that tiredness, headache, poor concentration and reduced productivity.2 In 2008, the Joint Task Force on Practice Parameters for Allergy and Immunology declared that “allergic rhinitis is a significant cause of widespread morbidity, medical treatment costs, reduced work productivity, and lost school days,” and that “…symptoms of may significantly affect a patient’s quality of life and can be associated with conditions such as fatigue, headache, cognitive impairment, and sleep disturbance.”15
Patients aren’t happy with current solutions
Health care practitioners typically assume that patients comply with all recommendation and prescriptions and that what they recommend as therapy works - if they don’t hear otherwise. However, in a study by Keith et al. in Canada, over 60% of patients reported that their symptoms were only somewhat, poorly or not controlled by their therapeutic regimen (figure 5), yet only 23% reported seeing a professional for allergy management in the past year.2
Figure 5: Level of control of symptoms as reported by patients who used various prescribed and OTC allergy treatments.
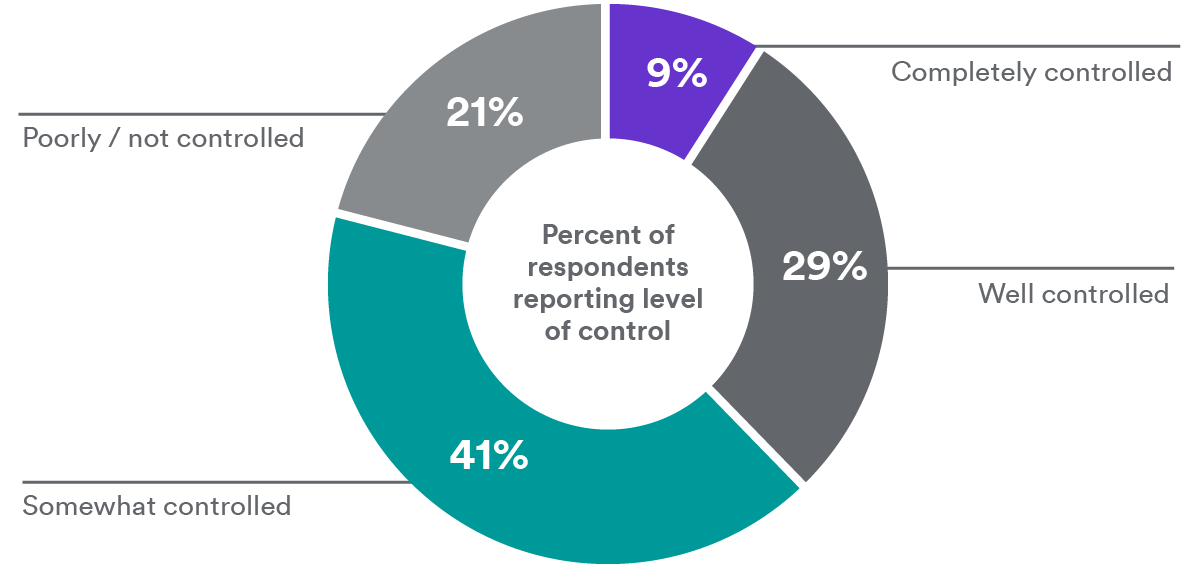
(Source: Keith 2012).
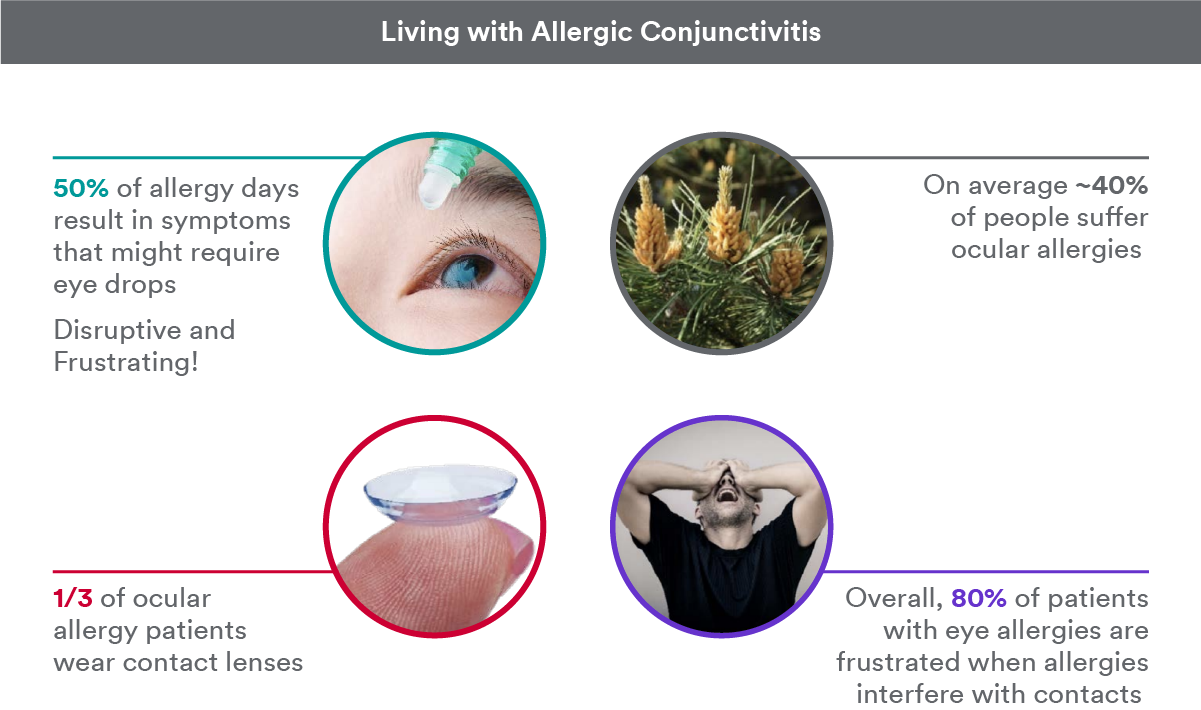
If we look at contact lens wearers in particular, allergic eye disease has been associated with disruptions to contact lens wear, following the expected seasonal and regional patterns – more prevalent in spring, summer and autumn, and the central, southeast and west/northwest regions of the US.16,17 In research commissioned by Johnson & Johnson Vision in 2015, an estimated 40% of US consumers suffer from ocular allergies, and over 1/3 of those are wearing contact lenses.18 A mobile ethnography survey was commissioned in 2018 that followed 150 contact lens-wearing allergy sufferers in the US and Japan during spring allergy season via mobile technology. The aim was to document the day-to-day experience of a contact lens wearer during allergy season, and better understand the impact of ‘bad’ allergy days. Subjects complete a short survey about themselves at the start of the process, daily check-ins for 2 weeks and a deep dive of 5 surveys on one day during allergy season. Nearly 80% of patients reported that wearing contact lenses was more uncomfortable during spring allergy season and that allergies disrupted their daily routine. A shocking 99% of ocular allergy sufferers experienced itchy eyes nearly all or most of the time they have symptoms. A common treatment for itchy eyes was eye drops, but over 50% of the time wearers felt drops were disruptive to their daily routine and over 8 in 10 were frustrated that allergies interfered with contact lens wear (Figure 6).18
Figure 6: Impact of allergies on contact lens wearers
Proactive communication is key
A recurring theme in medicine and patient care is the need for consistent, clear and frequent communication with patients about their condition. In the case of allergy management, the following communication points are imperative:
-
Interview patients about potential allergy symptoms at each and every visit – regardless of the time of year or prevailing pollen counts
-
Review in-office questionnaires for allergy symptoms
-
-
Ask “EVER” questions
-
Do your eyes ever itch?
-
Do you ever have allergies or hay fever?
-
Do you ever take allergy medicines (OTC or Rx)?
-
Do you ever forget to (or decide not to) take your medicines for allergies?
-
Do you ever find that your “once a day” medication doesn’t last all day?
-
-
Monitor pollen and mold counts in your area
-
Notify patients of upcoming pollen events/seasons
-
-
Stay current on adjunct therapies
-
Take an allergist or pharmacist to lunch!
-
-
Clearly explain treatments offered, including expectations around onset of action, duration of action and definition of and chances of success
-
Confirm patients know how to properly use treatment
-
-
Institute year-round social media campaigns
-
Educate regarding allergies
-
Inform patients (and other health care professionals) of your expertise
-